Public Health – Emerging / Reemerging Infections
Collective intelligence informs us that over the past 30 years, at least 30 new infectious diseases have emerged to threaten the health of millions of people across the globe – and has disrupted the security of nations.
As the greatest of all microbiologists of all (Louis Pasteur (1822-1895)) has said, “Gentlemen, it is the microbes that will have the last word” – indeed the World is more likely to experience the emergence of new infectious diseases as each year passes.
Scientific evidence is clear that approximately 60%-80% of all recognized human infectious diseases currently known of, and 75% of the emerging infections diseases that have affected humankind over the past 30 years, are Zoonotic in nature. The vast majority of these Zoonotic infections are the consequence of frequent interactions between humans, domestic animals and wildlife. Unfortunately, many of these diseases and microbes have had no specific treatment – and even worse – there has been a seriously limited scope of preventing or controlling these infectious spreads. As reported by the World Health Organization (WHO) infectious diseases constitute the 3rd leading cause of death worldwide.

The WHO also reports that Neglected infectious diseases, such as Diarrheal diseases and Malaria, cause for about 3 million deaths in children every year, and render at least 1 Billion people chronically infected. Cholera alone causes nearly 130,000 deaths a year worldwide (356 people dying every day). The Rota-virus is a major killer in both developed and developing countries, causing approximately 352,000- 592,000 deaths in children <5 years of age and 40% of diarrheal associated hospitalization in children <5 years of age worldwide. It appears that most of the emerging infectious diseases are caused by pathogens that are already present in the environment – they go unnoticed. What causes them to “emerge” is when the “conditions” change and become “favorable” for them to infect a new host. Sometimes, they simply “evolve” into a new variant and cause a new disease. Sometimes, both scenarios are present. The new and re-emerging pathogens that result are frequently resistant to any current form of treatment.
Accordingly, infectious diseases are continuously, and periodically, emerging, and re-emerging, in nearly every corner of the earth. Their ability to cause pandemics are accentuated by the ease of modern travel and the interconnectedness of the globalization.
The Global emergence of infectious diseases and associated deaths – have been alarming – and they have continued to expand across the globe ever since ancient times.
The Ongoing Mythology of Covid-19
It has has become ever more clear that the “elimination” of COVID-19 is a race against viral evolution – and the mythology of their treatments.
Weekly New Hospital Admissions of COVID-19

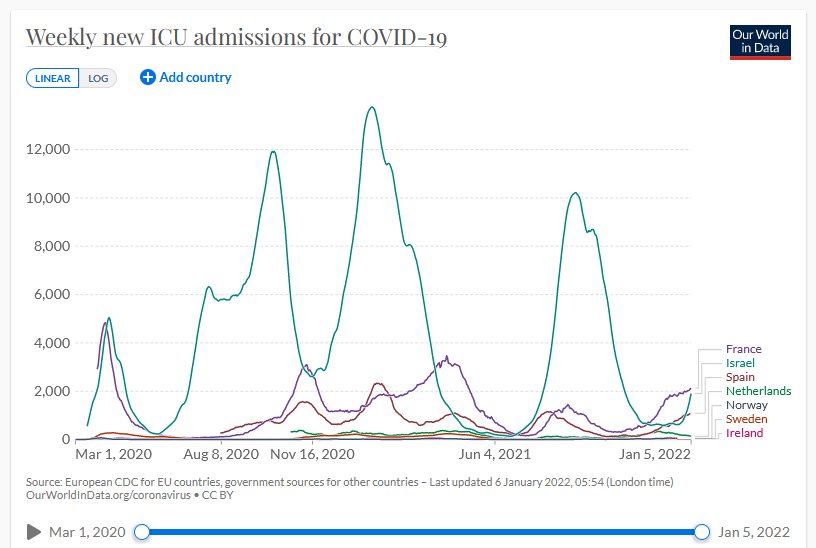
Weekly New ICU Admissions of COVID-19 Patients
No treatment, vaccine, or intervention is 100% available, nor effective, for all current and future variants. All practical, effective, and safe means should be used so as to not increase the risk of COVID-19 becoming ever endemic with increased morbidity and mortality.
While there are, of course, clearly substantial differences of professional opinion about the management of COVID-19 infections, the proper use of Ivermectin (IVM) has been promulgated by the Front Line COVID-19 Critical Care Alliance (FLCCC) (a group of highly trained and educated physicians) and has been exhaustively reviewed and commented upon.
In 2015, the Nobel Committee for Physiology or Medicine, in its ONLY award for treatments of infectious diseases since SIX (6) DECADES prior, honored the discovery of IVM. IVM is a multifaceted drug which has already been deployed against some of the world’s most devastating tropical diseases.
Since March 2020, when IVM was first used against a new global scourge, COVID-19, more than 20 randomized clinical trials (RCTs) have tracked IVM’s progress. Six of seven meta-analyses of IVM treatment RCTs reporting in 2021 found NOTABLE REDUCTIONS in COVID-19 FATALITIES, with a mean 31% relative risk of mortality vs. controls. During mass IVM treatments in Peru, excess Deaths Fell by a Mean of 74% over 30 days in its ten (10) states with the most extensive treatments. Reductions in deaths correlated with the extent of IVM distributions in all 25 states with p < 0.002.
The FLCCC publishes comprehensive protocols that are meant to work synergistically. Ivermectin is one of a number of evidence-based interventions but is not recommended alone. As we advance with our knowledge, experience and understanding through the pandemic, the Protocols have been updated .The FLCCC strongly advises against self-prescribing or use of animal forms of IVM.
The success of IVM requires early intervention – this appears to be almost universally true for ALL antiviral medications: Acyclovir (GlaxoSmithKline); Valacyclovir (GlaxoSmithKline); Remdesivir (Gilead); Tamiflu (Hoffmann-La Roche)
Molnupiravir (for new oral for Covid, Lagevrio, Molflu) (Merck) and Paxolovid (new oral for Covid Pfizer). The NIH utilizes the SAME category of recommendation with respect to IVM as they do for Monoclonal Antibodies Therapy (Remdesivir (Veklury); Tocilizumab (Acetemra) and Convalescent Plasma Covid-19 Therapy (the neutral “neither for or against” category thereby historically placing IVM’s use squarely within the reasonable judgment of a physician).
Clinical Outcomes
The literature is now full of articles favoring the use of IVM, both in prophylaxis and treatment of COVID-19. For favorable outcome on viral load and culture viability using IVM in early treatment of non-hospitalized patients with mild COVID-19 see a double-blind, randomized placebo-controlled trial at https://www.medrxiv.org/content/10.1101/2021.05.31.21258081v1.
Recent publications of note include a systematic review and meta-analysis by Bryant and Lawrie which found Clinically Significant Reduction in the risk of Death and moderate evidence of Substantial Reductions in Illness, and by Hill and Garrt: Hill A, Garrat A, et al. Meta-analysis of randomized trials of ivermectin to treat SARS-CoV-2 infection, Published by Oxford University Press on behalf of Infectious Diseases Society of America (https://pubmed.ncbi.nlm.nih.gov/34796244).
Hill and Grant’s review of 24 randomized trials found clinically significant reductions in death and inflammatory markers and improvements in clinical recovery: See also Morgenstern J. Redondo J. Olvarria A et al. Ivermectin as a SARS-CoV-2 Pre-Exposure Preventive in Healthcare Workers: a Propensity Score-Matched Retrospective Cohort Study available at: https://covid19criticalcare.com/wp-content/uploads/2021/09/IVM-as-a-Covid-Pre-Exposure-Preventive…pdf (74% Risk Reduction). See also Kory, P, Meduri, U, Iglesias, J et al. Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19, Am.J.Therapeutics. 2021; 28:3 – e299-e318.
Safety
According to the WHO, IVM is Safer Than both Aspirin and Tylenol. Its discoverer was honored with the Nobel prize for its global and historic impacts in eradicating endemic parasitic infections worldwide. Studies using IVM doses up to 10 times the FDA approved dose of 0.2mg/kg have not been associated with any increased adverse effects.
The COVID-19 Disease
COVID-19 is a highly heterogeneous and complex medical disorder. Without doubt, severe COVID-19 is probably amongst the most complex of medical conditions known. While we all try to understand the molecular pathways involved in patients infected with coronaviruses – we are still ALL constantly learning and evolving.
Fortunately we are enlightened by scholar scientists such as Marik et al who show us ways to understand the COVID-19 pathophysiology diagrammatically as seen below:

Published by Marik PE, Iglesias J, Varon J, Kory P. A., Scoping Review of the Pathophysiology of COVID-19. Int J Immunopathol Pharmacol. 2021 Jan-Dec;35:20587384211048026. doi: 10.1177/20587384211048026. PMID: 34569339; PMCID: PMC8477699.

Published by Marik PE, Iglesias J, Varon J, Kory P. A., Scoping Review of the Pathophysiology of COVID-19. Int J Immunopathol Pharmacol. 2021 Jan-Dec;35:20587384211048026. doi: 10.1177/20587384211048026. PMID: 34569339; PMCID: PMC8477699 as featured in International Journal of Immunopathology and Pharmacology
In Summary
Taking care of the healthcare of patients is a demanding profession which requires years of education, training and experience – it’s not something that can be replicated through short-cuts or through Dr. Google. Each individual is different, has a different set of co-morbidities, different circumstances, different states of pathophysiology, different medications and sensitivities, and different expectations. When it comes time to seek medical advice about complex medical conditions which may be life-threatening – seek proper medical consultation by someone who has the appropriate experience and wisdom to intervene on your behalf.
Public Health EmergenciesEpidemics / Pandemics |
||||
| Event | Deaths | Date | Location | Disease |
| Plague of Athens | 75,000-100,000 | 429-426 BC | Greece | Unkown |
| Antonine Plague | 5 – 7,000,000 | 165-190 | Roman Empire | Unkown |
| Plague of Justinian | 25-50,000,000 | 541-542 | Europe, Egypt, West Asia | Plague (40% of Population) |
| The Black Death | 20-200,000,000 | 1331-1353 | Europe, Asia, North Africa | Plague (60% of Population) |
| Cocoliztli Epidemic | 5-15,000,000 | 1545-1548 | Mexico | Salmonella |
| Italian Plague | 280,000 | 1629-1631 | Italy | Plague |
| Smallpox Plague | 1,000,000 | 1633-1634 | America | Smallpox; Killed 70% of Native American Population |
| Great Plague of London | 100,000 | 1665-1666 | England | Plague |
| Persian Plague | 2,000,000 | 1772 | Persia | Plague |
| Third Cholera Pandemic | 1,000,000 | 1852-1860 | Russia | Cholera |
| 1889 Flu Pandemic | 1,000,000 | 1889-1890 | Worldwide | Influenza |
| 1915 Encephalitis | 1,500,000 | 1915-1916 | Worldwide | Encephalitis lethargica |
| The Spanish Flu | 50,000,000 | 1918-1920 | Worldwide | Spanish Influenza Virus |
| Asian Flu | 2,000,000 | 1957-1958 | Worldwide | Influenza |
| Hong Kong Flu | 1,000,000 | 1968-1969 | Worldwide | Influenza |
| HIV/AIDS Pandemic | 35,000,000 | 1960-current | Congo; Worldwide | HIV Virus |
| 2009 Flu Epidemic | 203,000 | 2009 | Worldwide | Influenza |
| Ebola Virus Epidemic | 11,316 | 2013-2016 | West Africa | Ebola Virus |
| Zika Virus Epidemic | 53 | 2015-2016 | Worldwide | Zika Virus |
| 2002 SARS Coronavirus | 812 | 2002 | Worldwide | Coronavirus |
| 2009 Flu | 18,000 | 2009 | Mexico-USA-India | H1N1 Influenza A (67% of Deaths in USA) |
| 2012 MERS Coronavirus | 858 | 2012 | Middle East | Coronavirus; 34% Death Rate |
| 2019 Coronavirus Epidemic – COVID 19 | 3,128 | 2019-current | Worldwide | COVID-19 |
SARS – MERS – COVID 19
The WHO reports that the first Coronavirus epidemic occurred in 2002; it was known as Severe Acute Respiratory Syndrome (SARS). The 2002 SARS Coronavirus spread rapidly to 30 countries across Asia, the Americas, and Europe, with a total of 8,439 cases and 812 deaths – in less than a year.
The WHO identified the second Coronavirus in 2012; it was known as Middle East Respiratory Syndrome (MERS). Since 2012, 2,494 laboratory confirmed cases of MERS Coronavirus have been reported, and 858 associated deaths have occurred (34.4% case-fatality ratio). The MERS Coronavirus is still with us – there have been approximately 27 MERS deaths which have occurred as recently as the period between December 1, 2019 and January 31, 2020.
The current Coronavirus is closely related to the strain that caused the 2002 SARS outbreak, and is known as COVID 19. As of this writing, March 2, 2020, there have been 3,128 deaths due to COVID 19.

Our Approach
The Florida Medical Specialty Group, PA (FMSG) recognizes that despite emerging and re-emerging infectious diseases having demonstrated epidemic potential and massive health and economic risks, the global health community has largely failed to take a proactive approach to coping with outbreaks. In fact, more than 70% of the world remains under-prepared to prevent, detect, and respond to a public health emergency – especially one which involves infectious diseases. Preparing for epidemic threats requires constant education, preparation and training – because the environment from which these emerging and re-emerging infectious diseases is dynamic in an ever-changing world.
FMSG works with organizations such as healthcare institutions, private medical groups, complex business entities, and governmental agencies, to improve health outcomes for the people in greatest need globally who have been subjected to emerging and re-emerging infectious or serious public health risks. Our approach includes public health measures typically involving eliminating the pathogen from its reservoir, or from its route of transmission, ensuring a safe water supply, effectively managing sewage treatment and disposal, and initiating food safety, animal control, and vaccination programs.
FMSG works with you and your organization to assess your organization’s current public health and medical preparedness for public health risks and emergencies.
FMSG will review existing plans, policies, and procedures, identify necessary areas where corrective action may be necessary, and work with you to implement reasonable and cost-effective solutions to assure improved organizational and patient outcomes. We help prepare you, your staff, and your medical professionals, through education and training in public health risk management, to significantly improve your overall preparedness. Necessary topics may include incident command training, infection control, public health risks, contamination and de-contamination, non-toxic disinfection, the use of personal protective equipment (PPE), emergency preparedness and medical disaster management.

Our approach is: analysis – identification for opportunities to improve – implementation – education – training. This involves cycles of continuous evaluation and improvement. We specifically utilize our Pandemic Influenza Preparedness Program to assure your organization’s success, and your patient’s safety and improved outcome, in facing the emerging and re-emerging infectious disease public health risks and threats.

We understand that just as all public health risks and emergencies are not alike – all organizations are not alike. There is no one solution “fits all” when it comes to improving organizational and patient outcomes. Organizations have different and varying levels of experience and preparedness. Accordingly, we understand that some organizations may benefit most from our project management approach, while others may benefit most from our consulting, analysis, education and training programs.
Our intervention includes assuring organizational compliance with the tenants as delineated by the Centers for Medicare and Medicaid (CMS) with respect to Emergency Preparedness, Response, and Recovery. Our approach includes addressing increasing organizational viability; patient safety during emergencies; an “all hazards” risk assessment and coordinated responses to natural and man-made disasters; and addressing safeguarding human resources, maintaining business continuity, and protecting physical resources.